
PureTech Presents New Data from Phase 2b Open-Label Extension Study of Deupirfenidone (LYT-100), Further Supporting Strong and Durable Efficacy and Potential to Serve as New Standard of Care in IPF
Patients who switched from placebo or pirfenidone to deupirfenidone in the open-label extension study achieved stabilization of lung function with favorable tolerability
Findings further substantiate safety and efficacy results from the randomized, placebo- and active-controlled 26-week trial and highlight opportunity to address patients inadequately served by current therapies
Regulatory engagement underway; update on Phase 3 trial design expected in Q4 2025
BOSTON–(BUSINESS WIRE)–
PureTech Health plc (Nasdaq: PRTC, LSE: PRTC) (“PureTech” or the “Company”), a hub-and-spoke biotherapeutics company dedicated to giving life to science and transforming innovation into value, today announced new data from the open-label extension (OLE) of its Phase 2b ELEVATE IPF trial of deupirfenidone (LYT-100) in people living with idiopathic pulmonary fibrosis (IPF). These new results showed that participants who completed 26 weeks of placebo or pirfenidone treatment in the randomized portion of the trial and then switched to deupirfenidone for an additional 26 weeks in the OLE achieved stabilization of lung function. These findings, delivered in a late-breaking oral presentation at the 2025 European Respiratory Society (ERS) Congress in Amsterdam, Netherlands, highlight the potential for deupirfenidone to become a new standard of care for the treatment of IPF.
This press release features multimedia. View the full release here: https://www.businesswire.com/news/home/20250928954610/en/
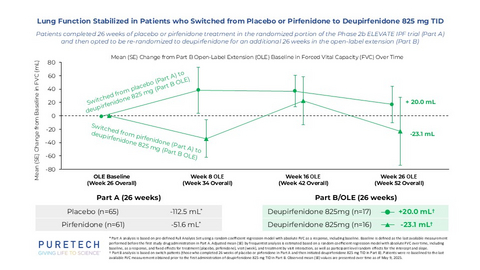
Lung Function Stabilized in Patients who Switched from Placebo or Pirfenidone to Deupirfenidone 825 mg TID
“The blinded portion of the ELEVATE trial challenged the perspective that the biggest opportunity for new therapies in IPF is improved safety, by showing that treatment with deupirfenidone 825 mg three times a day can achieve lung function stabilization with favorable tolerability. The initial 52-week extension data then raised the bar by demonstrating that this effect with deupirfenidone was durable,” said Argyrios E. Tzouvelekis, M.D., Ph.D., University of Patras, Greece, and presenting investigator at ERS 2025. “Now we are seeing that two additional patient cohorts who experienced lung function decline in Part A of the trial achieved stabilization once switched to deupirfenidone. These findings reinforce that the blinded results with deupirfenidone are reproducible and support the potential for benefit in patients transitioning from standard of care.”
ELEVATE IPF, a global, randomized, double-blind, active- and placebo-controlled Phase 2b trial, achieved its primary endpoint and demonstrated a statistically significant and clinically meaningful reduction in lung function decline at 26 weeks with deupirfenidone 825 mg three times a day (TID) compared to placebo (Part A). As previously announced, participants treated with deupirfenidone 825 mg TID experienced a slower rate of lung function decline, as measured by change from baseline of Forced Vital Capacity (FVC), at 26 weeks versus those who were treated with pirfenidone 801 mg TID or placebo (-21.5 mL vs. -51.6 mL vs. -112.5 mL, respectively), with a 91 mL difference between deupirfenidone 825 mg and placebo at 26 weeks. Following the completion of the blinded portion of the trial, 170 participants (more than 90%) enrolled in the OLE (Part B). Those who remained on deupirfenidone 825 mg TID maintained a robust treatment effect and experienced an overall FVC decline of -32.8 mL over the 52-week period,1 which is similar to the expected natural decline in lung function in healthy older adults over that time (approximately -30.0 mL to -50.0 mL).2
The new results presented at ERS provide additional evidence from participants who initially received placebo or pirfenidone for 26 weeks during Part A and then switched to deupirfenidone for 26 weeks in Part B. Those who switched from placebo to deupirfenidone 825 mg TID (n=17) had a mean change in FVC of +20.0 mL (placebo switch cohort), while those who switched from pirfenidone to deupirfenidone 825 mg TID (n=16) had a mean change in FVC of -23.1 mL (pirfenidone switch cohort).3 These results provide further evidence from two additional patient cohorts that deupirfenidone may stabilize the decline in lung function to that expected of healthy older adults and suggest a potential benefit for patients transitioning from standard of care to deupirfenidone.
Deupirfenidone continued to be well tolerated at both doses studied in Part B after six months of treatment, and the safety profile remained consistent with Part A. Additional analyses shared at ERS included a summary of the most common treatment-emergent adverse events (TEAEs) in the OLE, defined as occurring in at least 10% of participants in either treatment group. As of May 9, 2025, the most common TEAEs were nausea (8.4% vs. 11.5%), dyspepsia (14.5% vs. 12.6%), upper respiratory infections (16.9% vs. 17.2%), and cough (10.8% vs. 4.6%) for deupirfenidone 550 mg TID (n=83) and deupirfenidone 825 mg TID (n=87), respectively.
“The ELEVATE trial has been designed and executed to provide one of the most rigorous Phase 2 evaluations of a potential therapy in IPF,” said Sven Dethlefs, Ph.D., Chief Executive Officer of Celea Therapeutics, the PureTech Founded Entity created to advance deupirfenidone. “The reproducibility we’re seeing across blinded and extension data, and now in switch cohorts, gives us strong confidence in the robustness of the findings. We believe deupirfenidone has the potential to become a new standard of care in IPF, and we are actively engaging with regulators to finalize the Phase 3 trial design and expect to share an update in the fourth quarter.”
About Deupirfenidone (LYT-100)
Deupirfenidone (LYT-100) is in development as a potential new standard of care for the treatment of idiopathic pulmonary fibrosis (IPF). It is a deuterated form of pirfenidone, which – along with nintedanib – is one of the two FDA-approved treatments for IPF. Both approved therapies offer only modest efficacy in slowing lung function decline, largely due to tolerability challenges that limit the ability to achieve higher doses that could significantly improve patient outcomes. These limitations have contributed to low treatment uptake and poor adherence, with approximately 25% of people with IPF in the U.S. ever receiving either drug.4 Despite this, combined peak global sales exceed $5 billion, representing a significant market opportunity in IPF and other fibrotic lung diseases. 5
Deupirfenidone may overcome these limitations. In the global Phase 2b ELEVATE IPF trial, deupirfenidone demonstrated the potential to stabilize lung function decline over at least 26 weeks as a monotherapy while maintaining a favorable safety and tolerability profile. Initial data from an ongoing open-label extension study suggest that this effect may be sustained through at least 52 weeks. These findings support the potential for deupirfenidone to offer a meaningful advance for people living with this progressive and deadly disease. Beyond IPF, deupirfenidone may also address multiple underserved fibrotic conditions, including progressive fibrosing interstitial lung diseases.
About Idiopathic Pulmonary Fibrosis (IPF)
Idiopathic pulmonary fibrosis (IPF) is a rare, progressive, and fatal lung disease characterized by irreversible scarring of lung tissue that leads to a steady decline in lung function. Median survival following diagnosis is estimated to be two to five years, and currently there is no cure.6
About Celea Therapeutics
Celea Therapeutics is dedicated to advancing transformative treatments for people with serious respiratory diseases. Drawn from the Latin word for “sky,” the name reflects the company’s mission to rise above the status quo and deliver therapies that change lives. The company’s lead program, deupirfenidone (LYT-100), is a Phase 3-ready therapeutic candidate with the potential to set a new standard of care for idiopathic pulmonary fibrosis (IPF) and other fibrotic lung diseases.
Celea was founded by PureTech Health plc (Nasdaq: PRTC, LSE: PRTC), a biotherapeutics company dedicated to giving life to science. PureTech’s innovative R&D model drives the creation of Founded Entities like Celea, enabling the advancement of highly promising medicines to patients in a capital-efficient manner. For more information, please visit www.celeatx.com and www.puretechhealth.com.
About PureTech Health
PureTech Health is a hub-and-spoke biotherapeutics company dedicated to giving life to science and transforming innovation into value. We do this through a proven, capital-efficient R&D model focused on opportunities with validated pharmacology and untapped potential to address significant patient needs. This strategy has produced dozens of therapeutic candidates, including three that have received U.S. FDA approval. By identifying, shaping, and de-risking these high-conviction assets, and scaling them through dedicated structures backed by external capital, we accelerate their path to patients while creating sustainable value for shareholders.
For more information, visit www.puretechhealth.com or connect with us on X (formerly Twitter) @puretechh.
Cautionary Note Regarding Forward-Looking Statements
This press release contains statements that are or may be forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. All statements contained in this press release that do not relate to matters of historical fact should be considered forward-looking statements, including without limitation statements that relate to continued development of and regulatory interactions related to deupirfenidone, the potential of deupirfenidone in IPF and other indications, our expectations around our therapeutic candidates and approach towards addressing major diseases, our plans to advance our programs and deliver on our milestones, our future plans, prospects, developments, and strategies. The forward-looking statements are based on current expectations and are subject to known and unknown risks, uncertainties and other important factors that could cause actual results, performance and achievements to differ materially from current expectations, including, but not limited to, those risks, uncertainties and other important factors described under the caption “Risk Factors” in our Annual Report on Form 20-F for the year ended December 31, 2024 filed with the SEC and in our other regulatory filings. These forward-looking statements are based on assumptions regarding the present and future business strategies of the Company and the environment in which it will operate in the future. Each forward-looking statement speaks only as at the date of this press release. Except as required by law and regulatory requirements, we disclaim any obligation to update or revise these forward-looking statements, whether as a result of new information, future events or otherwise.
| ____________________________ |
| 1 Integrated analysis of double-blind (26 weeks) and initial open-label extension data from Phase 2b ELEVATE IPF trial as of May 9, 2025, using a random coefficient regression model with absolute FVC including baseline as response variable and week, treatment and interaction between week and treatment as fixed effect. The analysis was performed based on the predefined Full Analysis Set. |
|
2 Valenzuela, C., Bonella, F., Moor, C., Weimann, G., Miede, C., Stowasser, S., & Maher, T. (2024, September). Decline in forced vital capacity (FVC) in subjects with idiopathic pulmonary fibrosis (IPF) and progressive pulmonary fibrosis (PPF) compared with healthy references [Poster presentation]. European Respiratory Society International Congress, Vienna, Austria; and Luoto, J., Pihlsgård, M., Wollmer, P., & Elmståhl, S. (2019). Relative and absolute lung function change in a general population aged 60–102 years. European Respiratory Journal, 53(3), 1701812. https://doi.org/10.1183/13993003.01812-2017 |
| 3 Part B analysis is based on switch patients (those who completed 26 weeks of placebo or pirfenidone in Part A and then were re-randomized to receive deupirfenidone 825 mg TID in Part B). Patients were re-baselined to the last available FVC measurement obtained prior to the first administration of deupirfenidone 825 mg TID in Part B. Observed mean (SE) values are presented over time as of May 9, 2025. |
| 4 Dempsey, T. M., Payne, S., Sangaralingham, L., Yao, X., Shah, N. D., & Limper, A. H. (2021). Adoption of the antifibrotic medications pirfenidone and nintedanib for patients with idiopathic pulmonary fibrosis. Annals of the American Thoracic Society, 18(7), 1121–1128. |
| 5 Esbriet peak sales (2020) per Roche 2021 Financial Results & Ofev peak sales (2024) per Boehringer Ingelheim 2024 Financial Results. Ofev sales include those for all approved indications – IPF, PF-ILD, and systemic sclerosis-associated interstitial lung disease (SSc-ILD). |
|
6 Fisher, M., Nathan, S. D., Hill, C., Marshall, J., Dejonckheere, F., Thuresson, P., & Maher, T. M. (2017). Predicting life expectancy for pirfenidone in idiopathic pulmonary fibrosis. Journal of Managed Care & Specialty Pharmacy, 23(3-b Suppl), S17–S24. https://doi.org/10.18553/jmcp.2017.23.3-b.s17 |
View source version on businesswire.com: https://www.businesswire.com/news/home/20250928954610/en/
PureTech
Public Relations
[email protected]
Investor Relations
[email protected]
UK/EU Media
Ben Atwell, Rob Winder
+44 (0) 20 3727 1000
[email protected]
US Media
Justin Chen
[email protected]
KEYWORDS: Europe United States Netherlands North America Massachusetts
INDUSTRY KEYWORDS: Oncology Health FDA General Health Clinical Trials Pharmaceutical Biotechnology
MEDIA:
| Photo |
 |
| Lung Function Stabilized in Patients who Switched from Placebo or Pirfenidone to Deupirfenidone 825 mg TID |
| Logo |